PULMONARY HYPERTENSION
“It’s because of patients like Jenna that we’ve been able to improve our treatment for things like pulmonary hypertension”

VIDEOS

Pulmonary Hypertension Explained: Animation
Pulmonary Hypertension Treatment Explained - Guidelines
Successfully Managing Pulmonary Hypertension
Educational Video: Living With Pulmonary Hypertension

Center for Lungs and Breathing
Pulmonary Hypertension Treatment Options | Temple Health
Pulmonary Arterial Hypertension: Signs, symptoms and support

Pulmonary Rehab: Daily Fitness & Exercise

Beathing exercises for strong lungs
It’s important to keep yourself empowered and informed a a patient so be sure to join the PH Associations and stay up-to-date with new information, new research and new treatment options.
What is Pulmonary Arterial Hypertension?
The reading matter on PH can be confusing and dense, so we have tried to simplify it as much as possible. Some of the information is specific to Jenna’s journey; if you want more of the medical speak, simply Google ‘primary pulmonary hypertension’ or ‘primary arterial hypertension’.
How Common is PH?
PH has an annual incidence of one to two cases per million people in
the US and Europe. It is two to four times as common in women as in
men. The mean age at diagnosis is around 45 years, although the
onset of symptoms can occur at any age. In short, it can strike
anyone.
“For me, it’s really important that people don’t suffer like I did in terms of having a really extended diagnosis, because that means that once you get diagnosed, there is a limited amount that you can do to claw your way back to health”~ JENNA LOWE
What are the Symptoms of PH?
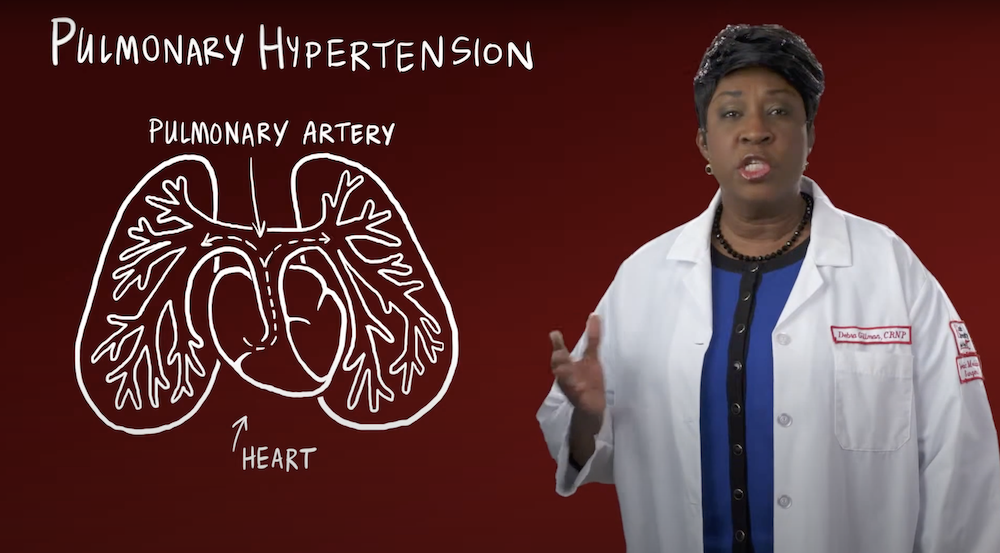
The symptoms are caused by extremely high blood pressure in the veins and arteries of the lungs only (not to be confused with high blood pressure in the whole body), which restricts blood flow through the lungs. This results in increased stress on the heart and compromised blood circulation through the whole body, owing to decreased cardiac output and low oxygen saturation.
What causes PH?
The exact cause behind the development of PH is not known. However, research has led to a better understanding of underlying pathological mechanisms. PH is recognised as a complex, multifactorial condition involving numerous biochemical pathways and different cell types.
Treatment of PH
Not so long ago, there were no treatments for PH and the prognosis was one to three years. This has recently changed and there are many drugs on the market to help prolong life expectancy. The earlier you’re diagnosed, the better your chances are of enjoying a longer life.
VIDEOS
Pulmonary Hypertension Explained: Animation
Pulmonary Hypertension Treatment Explained - Guidelines
Successfully Managing Pulmonary Hypertension
Educational Video: Living With Pulmonary Hypertension
Center for Lungs and Breathing
Pulmonary Hypertension Treatment Options | Temple Health
Pulmonary Arterial Hypertension: Signs, symptoms and support
Pulmonary Rehab: Daily Fitness & Exercise
Beathing exercises for strong lungs
It’s important to keep yourself empowered and informed a a patient so be sure to join the PH Associations and stay up-to-date with new information, new research and new treatment options.
Quick facts - Things you need to know

Organ Donation
Even though SA is the home of the first ever heart transplant less that 0.3% of our population are organ donors. On any one given day there are at least 4,300 people awaiting an organ transplant. It is quick, easy and costs nothing to become a donor. Your organs could save up to seven lives when you die.

Rare Diseases
Did you know that over 7,000 different rare diseases have been identified to date, directly affecting the daily life of more than 350 million people worldwide? The complex nature of rare diseases, coupled with limited access to treatment and services, means that family members are often the primary source of solidarity, support and care for their loved ones. The Rare Disease Society of SA has become a crucial source of information, experience and resources for families affected by rare diseases in South Africa.

Pulmonary Hypertension
Pulmonary Hypertension is a progressive, degenerative disease caused by the narrowing or tightening of the veins and arteries in the lungs. Common early symptoms of PH include: Breathlessness (particularly during physical activity); excessive fatigue; dizziness; fainting; peripheral oedema and chest pain (particularly during physical activity).
Quick facts
Things you need to know
Organ Donation
Even though SA is the home of the first ever heart transplant less that 0.3% of our population are organ donors. On any one given day there are at least 4,300 people awaiting an organ transplant. It is quick, easy and costs nothing to become a donor. Your organs could save up to seven lives when you die.
Rare Diseases
Did you know that over 7,000 different rare diseases have been identified to date, directly affecting the daily life of more than 350 million people worldwide? The complex nature of rare diseases, coupled with limited access to treatment and services, means that family members are often the primary source of solidarity, support and care for their loved ones. The Rare Disease Society of SA has become a crucial source of information, experience and resources for families affected by rare diseases in South Africa.
Pulmonary Hypertension
Pulmonary Hypertension is a progressive, degenerative disease caused by the narrowing or tightening of the veins and arteries in the lungs. Common early symptoms of PH include: Breathlessness (particularly during physical activity); excessive fatigue; dizziness; fainting; peripheral oedema and chest pain (particularly during physical activity).


How to HelpMake a difference right now
PROUD TO
PARTNER WITH



Proud to partner with:
PROUD TO
PARTNER WITH

Jenna Lowe’s parents continue her mission to campaign for organ donation awareness in SA
.png)
Even during her last six months, Jenna was calm and extraordinary’
.png)